is original antigenic sin starting to dominate covid?
the data is starting to look alarming
 |

the good news is that omicron looks mild.
the bad news is that it increasingly looks like the variant that original antigenic sin (OAS) begot and this means that the vaccinated may be wide open for it in a way they would not have been had these programs not been rolled out. worse, they may NEVER be able to generate sound immunity because that’s what OAS does.
if OAS really is taking hold, we’re going to keep seeing more and more of this:



if this is what it looks like to me, this is not spreading like wildfire in these groups because omicron is some crazy new superspread variant. it’s spreading because all these people over-trained their immune systems against a specific spike protein pattern and their immune response is now a one trick pony that cannot mount an effective sterilizing resistance against variants and perhaps will NEVER gain this capability.

let’s take it from the top:
OAS is very real. people act like it’s some fanciful idea, but this is because they have never dug into immunology. this has been studied deeply and has been a major issue in flu for ages.
it’s really a pretty simple idea that likely suffers unwarranted skepticism owing to a name that makes it sound like some sort of faith healing concept.
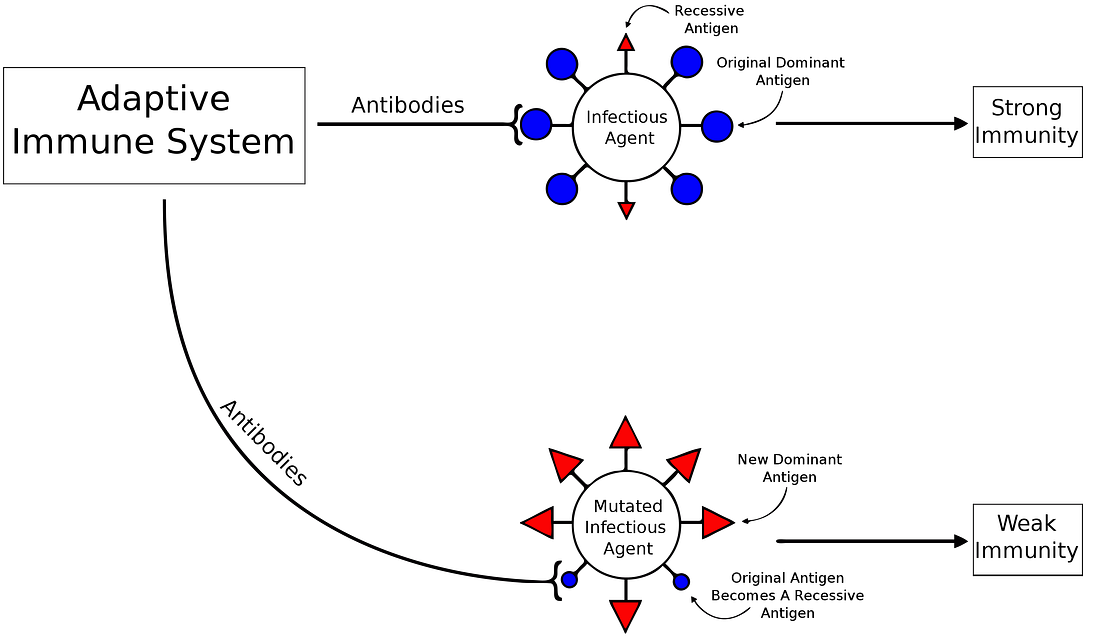
your immune system is adaptive. it experiences pathogens and learns to recognize and respond to them. but the diversity of response is not unlimited.
you experience a flu one year, then another the next. if they are sufficiently similar, you may just use the same antibodies you used last year (or 20 years ago). they are unlikely to work as well because they are not specific to this new virus. if they diverge sufficiently, you could be in real trouble. you’ll be spamming a response that has no effect and forgoing those that do. the virus can run rampant. (DETAIL)
and we’ve seen some of this in covid already.
gatopal™ eugyppius with whom i’ve had some good discussion on this had a great piece on it yesterday:

some key takeaways:
“They found that the immune response of the severely ill, unlike that of the mild patients, was dominated by IgG antibodies against ordinary seasonal coronaviruses. In other words, the most severely ill patients had fewer naive B cells imprinting on SARS-CoV-2, and more memory B cells producing antibodies against the somewhat similar common coronaviruses these patients had recovered from in the past…”
that’s OAS.
it was shown again in mice:
what this is telling you is simple: some kinds of previous coronavirus exposure made you less able to fight off covid 19, while others did not. exposure to covid itself left you highly competent to respond next time.
(this is likely the explanation for the low pacific rim covid counts from early variants that then exploded around delta (and will on omi). it was biome specific immunity that wound up getting evaded.)
 this dovetails into the data discussed the other day (
this dovetails into the data discussed the other day (
HERE) about the order of vaccination and infection mattering in terms of ultimate immunity.
getting vaccinated first then recovering is less protective than just recovering or of recovering and then getting vaccinated.
risk is up about 23% vs recovered alone and a whopping 48% from having had coivd then vaxxing (though the absolutely numbers are small. this was a young, healthy test population. how it might fare in the older and more infirm remains an open question)
that too smacks of strongly OAS. this is, if not a smoking gun, at least a gun with a hot barrel.

much has been made of the “high antibody” levels produced by the vaccines. they are, in fact, much higher than the levels from actual covid infection. but is more really more? there is actually no evidence that this is so. increasingly, it appears to be the opposite. these levels are too high.
not only does this lead to more prevalent and more severe side effects, but there is no demonstrated link to better clinical outcomes from these sky high early levels.
potentially worse, there really looks to be a link to immuno-overtraining and exactly the sort of narrow rather than broad response that characterizes original antigenic sin.
this is just how that pathway manifests. failure to respond to nucleocapsid will not only render response weaker, it may prevent the development of sterilizing immunity altogether and that could wind up being permanent.
the vaccines for covid have already been failing on stopping spread. the data from the UK (which seems to be the highest quality and most thorough in the world) has been showing this for ages. the vaccinated are getting covid at far higher rates than the unvaxxed.
(effective VE added in red by me)
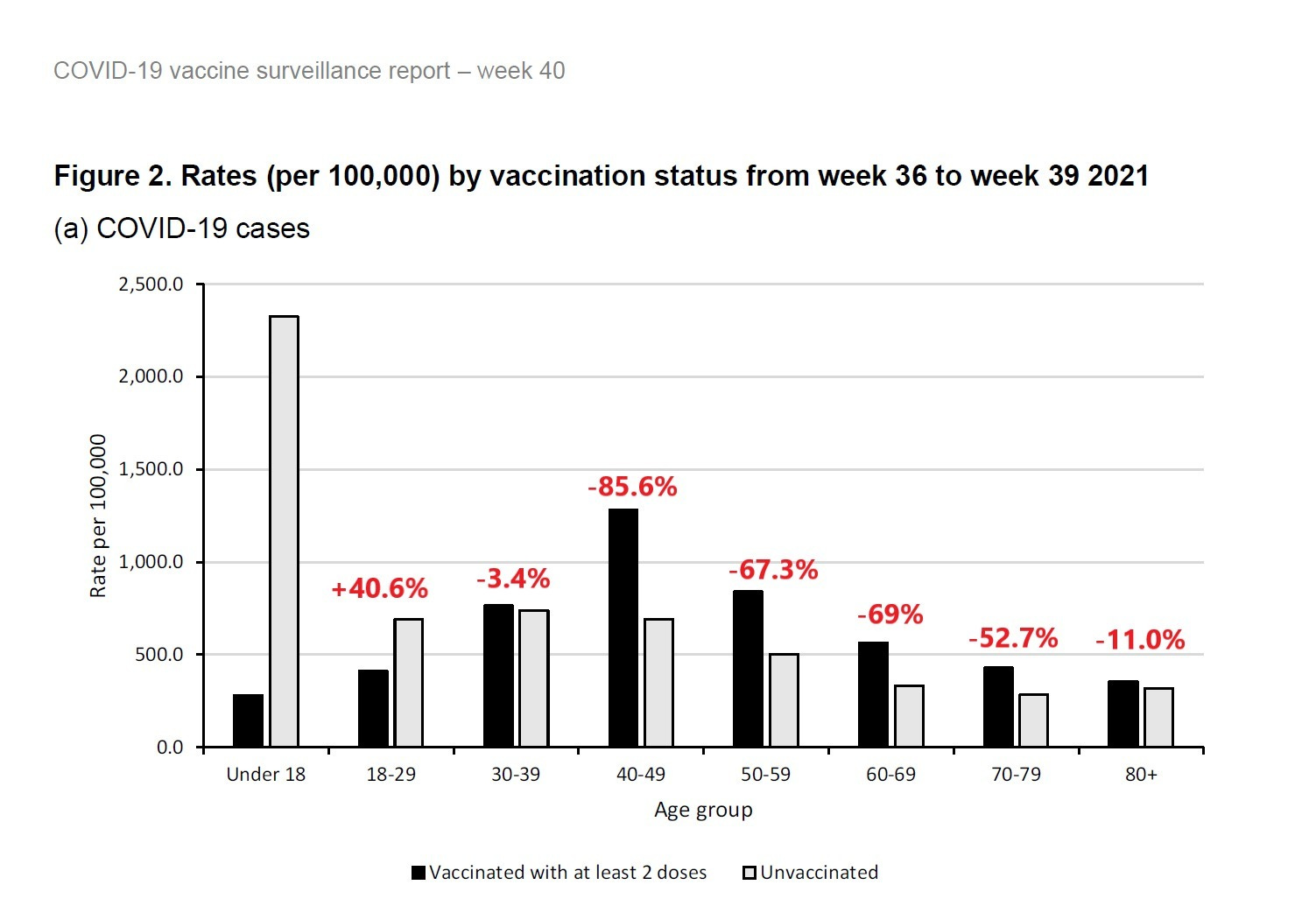
if omicron is emerging as a more OAS optimized variant more able to evade the narrowly trained spike response from the mRNA and adenovirus vaccines, then it’s going to run like wildfire through the vaxxed.
the idea that boosters represent a solution will be shown to be exactly wrong. that’s going to provide one of the interesting acid tests here and looks to be the data you want to track to assess this hypothesis.
initial DATA is still a bit anecdotal and need to be handled and assessed as such, but it’s also looking awfully consistent as well and these are a lot of compass needles to all be pointing in one direction to ignore.
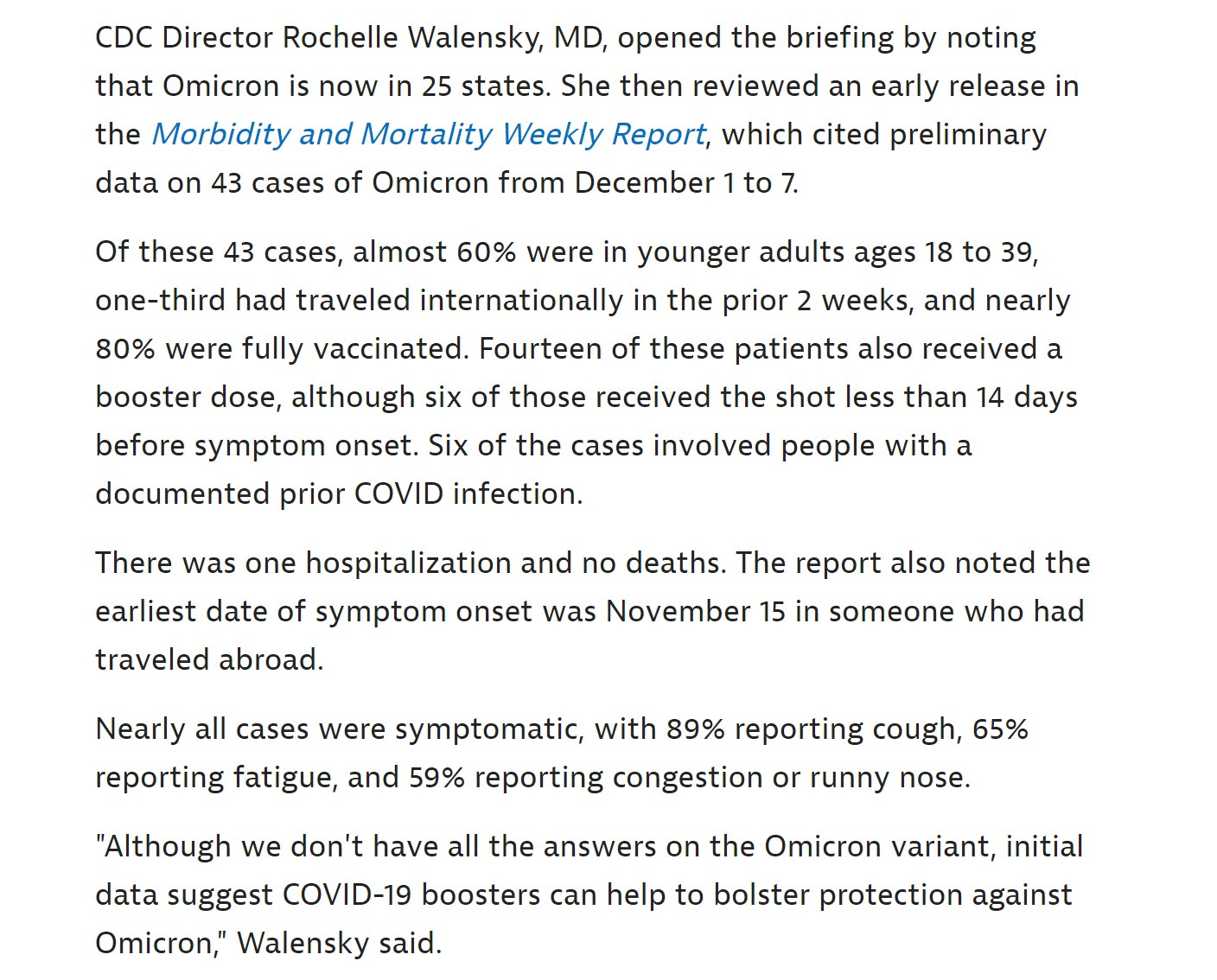
“Walensky also reiterated that over 99% of COVID cases in the U.S. are from Delta, and Omicron accounts for less than 0.1% of current cases.”
the US has not really seen omi yet. it’s here, it’s running around, but the current crop of results are still delta.
but of these 43 cases, 80% were vaxxed (and i’m sure they’re using the fully double vaxxed +2 weeks definition there) so that’s way above the US population avg of 60% (though the sample might be skewed by selection bias for travelers).
14 had a booster. that’s a full 1/3.
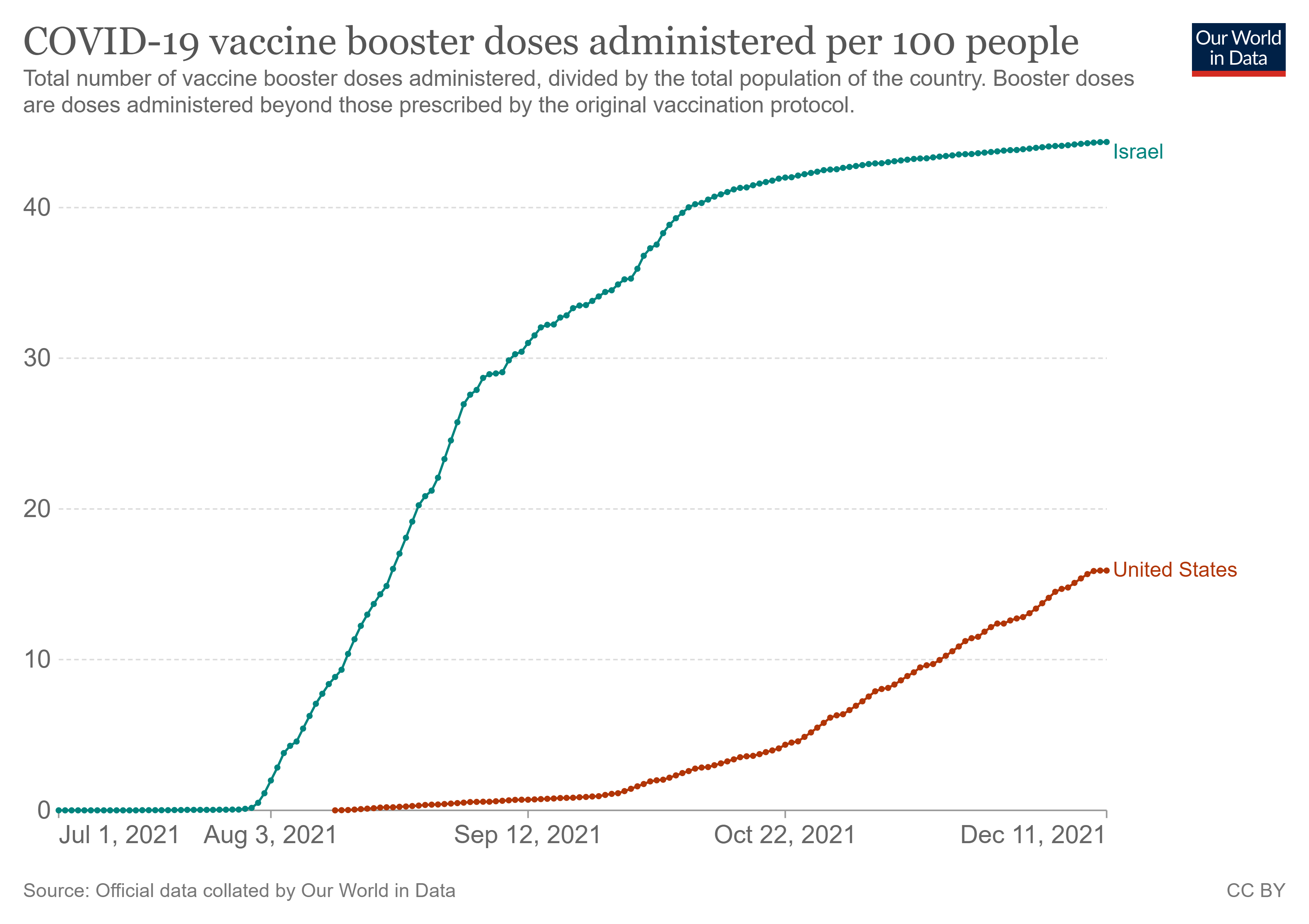
davi’s data above showed 76% of omi cases in israel were in the boosted.
i don’t know where he’s getting that 70% boosted number for israelis though.
OWID seems to think it’s considerably lower. (anyone have a definitive read?)
the group i get REALLY interested in are the 6 with prior infection. based on the data from above, it seems like we really want to know if they were also vaxxed and in what order they got vaxxed an infected.
if they seem to disproportionately be vaxxed then infected prior to re-infection, that would be a strong pointer to OAS issues.
this is important data to run down because it has widespread and counter narrative implications.
if OAS is now dominating covid it implies that vaccinating kids who have not had covid could be setting them up for a lifetime of inability to generate strong, sterilizing covid immunity.
this same logic applies to basically any healthy adult.
vaccination post covid does not seem to carry this risk (so far) but boosters might tip that over time. (or perhaps not) in any event, the incremental absolute gain is so low that it makes vaccines look unattractive for any but the very highest risk to vaxx post infection.
will keep tracking this as it’s going to be the thing to know in coming months and if this pans out, whether it’s omi or not, we’re going to see the OAS variants hit.
it is, of course, still possible i’m wrong here (and frankly, i’d like to be because this is NOT good), but this sure starting to walk and quack a lot like a duck to not be a waterfowl…
Source: bad cattitude
No comments:
Post a Comment